A 60 Y Male chronic alcoholic presented to the OPD with distended abdomen
12th July 2023
NOTE: THIS IS AN ONLINE E LOGBOOK TO DISCUSS OUR PATIENT'S DE-IDENTIFIED HEALTH DATA SHARED AFTER TAKING HIS/HER GUARDIAN'S SIGNED INFORMED CONSENT. HERE WE DISCUSS OUR INDIVIDUAL PATIENT'S PROBLEMS THROUGH A SERIES OF INPUTS FROM THE AVAILABLE GLOBAL ONLINE COMMUNITY OF EXPERTS INTENDING TO SOLVE THOSE CLINICAL PROBLEMS WITH COLLECTIVE CURRENT BEST EVIDENCE-BASED INPUT.
This is the case of a 60 year old male farmer and carpenter by occupation and resident of Guramguda. The following history was taken with the patient in person. The patient was explained about confidentiality and written consent was taken to create the following case report.
This case report aims to record the patient's journey.
CHIEF COMPLAINTS:-
-Abdominal distension since 4months
-Swelling of bilateral lower limbs since 4 months
-decreased urine output since 4months.
History of present illness:-
Patient was apparently asymptomatic 4months back. He then developed abdominal distension which is insidious in onset and associated with pain which is stabbing type ,aggravated on eating and no relieving factors.
-H/O swelling in both legs upto level of knees associated with dragging type of pain since 4months.
-H/O decreased urine output since 4months.
-H/O SOB since 4months
-Patient then went to a hospital and on medication complaints were subsided. He developed the same complaints 10days back and came to the our OPD hospital yesterday(i.e 7th july 2023).
-H/O chronic cough since 4months with whitish sputum.
-H/O burning micturition since 1month.
-H/O intermittent fever since 10 days associated with chills and rigors relieved on medication.
-Other complaints- presence of spherical swelling insidious in onset (1month ago) infront of leg 9inches from the lower border of patella initially in the size of a peanut and progressive to the current size measuring 3x3cm. The swelling is tender, firm in consistency and no mobility and punctum is seen.
History of past illness:-
H/O 2episodes of seizures 12years ago controlled by medication.
H/O spasms of both limbs phalanges
K/C/O Type 2 DM and HTN since 6years.
N/K/C/O- TB, asthma, CVA , CAD , Thyroid disorders.
Surgical history
Cataract removal for one eye 2years ago and other eye 1year ago.
Removal of cyst like swelling present between two eyebrows 1year ago.
H/O blood transfusion done 3months back-uneventful
Personal history:-
Water intake:- half a litre per day
Appetite:- decreased appetite since two months
Diet:- mixed
Bowel movement:- H/O constipation since 1 month, passing stools once in 3days.
Bladder movement:- decreased urine output since 4months with burning micturition since 1month.
Alcohol:- Chronic alcoholic since 40years(around 180ml/day)
Smoking:- chronic smoker since 40years(one pack of beedi per day containing 18 beedis)
Addiction:- nil
Allergies:- nil
Exercise status:- moderate
FAMILY HISTORY:-
- not significant.
PHYSICAL EXAMINATION:-
GENERAL EXAMINATION:-
The examination was conducted at a well lit and well ventilated room. The patient was conscious, cooperative and coherent.
Moderately built
Afebrile
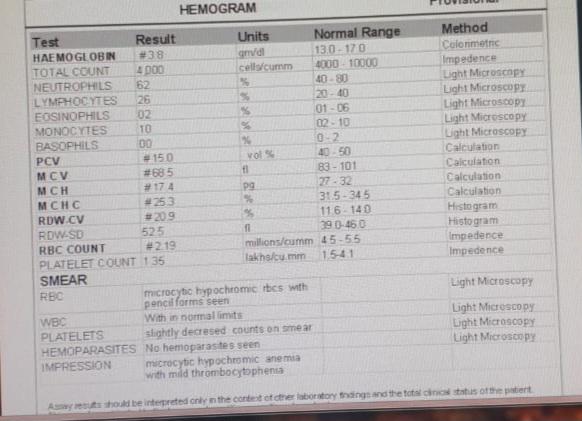
Pallor present

No Icterus
No Cyanosis
No Clubbing.
Bipedal edema -present pitting type

No Significant lymphadenopathy

VITALS:
Temp- Afebrile
BP-140/70
PR-105bpm
RR-24cpm
Spo2-96% at room air
GRBS:485mg/dl
SYSTEMIC EXAMINATION:
CVS:
Inspection -
Chest wall is bilaterally symmetrical
Ne precordial bulge is seen
Palpation-
JVP- Normal
Apex beat-palpated in 5th intercostal space in mid clavicular line
Auscultation-
S1&S2 are heard
No murmurs
RESPIRATORY SYSTEM:






















Comments
Post a Comment